MTF HRT Suggestions From A Fellow Transfem
 • 15 minutes read •
• 15 minutes read •
This article touches on some aspects of sex ed
Okay so the way this post is gonna work is
This is not medical advice, these are medical opinions.
I am going to start with simple, easy wins, nearly objective facts, and get into personal opinions and hypothetical territory as I go along, hopefully sign post it as we go.
These medical opinions are for the inquistive potential transfeminine individuals and nonbinary pals wanting some feminine traits, but focusing on individuals who want As Much Femininity As Possible As Fast As Possible. Nonbinary transfem pals click here This advice comes from and thus is primarily meant for the american market, your local situation may be different. Also, not a doctor, just a transfem who has been using and researching for a couple years.
Obvious out of the way, transfem individuals will take estradiol to receive feminine traits and lessen masculine ones. Hormone Replacement Therapy. The goal is typically to reduce testosterone and raise estradiol. US healthcare safe fields for this and normal hormone levels to aim for will be 100-400pg/mL estradiol (100+ simply gaurantees feminization) and 15-75ng/dL testosterone. Tested normally at “trough”, the 6th day of 7 day injection cycle. Transfems will usually start at near 0 estradiol and 400-600 testosterone at the beginning of therapy/before therapy. We’re decently sure that too high of levels of estradiol are harmful, even on extremely safe HRT injections. [x]
(Really too high or too low of both testosterone and estrogen is bad, it is a balancing act, not a high score To Win)
Noted and potentially wanted effects:
- breast growth
- No male pattern baldness if started soon enough before balding
- soft skin
- less oily skin/hair (sometimes reduces acne)
- reduced libido/spontaneous erections/semen (Your libido will usually return, eventually, and be changed for how it acts)
- Genital shrinkage/atrophy if not Used
- Will usually kill your sperm count (freeze it if you want it)
- thinning of body hair folicles (YOU WILL STILL GROW IT)
- Face shaping, fat redistribution (Hips)
- (subjectively) emotional changes/confidence changes/sexuality changes [x], lessens depression, lessens brainfog
Injections
(or How I learned to stop worrying and love the stab)
First, easily:
https://startwith4mgestradiolenanthateweeklyandtestatonetothreemonths.com/
Start with 4mg of Estradiol Enanthate injections Weekly And Test E and T At 3 Months.
Enanthate is by far the best form of estrogen we currently have on the market, with very little downsides or risks to speak of, it suppresses testosterone on its own, and no anti-androgen or additional medicine is needed. (Cypionate and Valerate injections also do this, with some small caveats) The dosage is very average across the board, but you may have to raise or lower it depending on blood levels none the less, you test your blood levels because everyone is different and your body might EAT or REJECT estrogen more than others.
Needle fear is a problem, but the vast majority of people can conquer their needle fear with a few injections done. (Injections are easier and less painful than routine blood work, I promise you) If you particularly struggle with needle fear, agony/freezing/running, you know to search out other medicine. I recommend going from top down for options.
Injections > Gels/Patches > Sprays > Pills. [x]
Estradiol Enanthate is currently illegal in the USA due to simply not going through the FDA yet and probably not going through for the foreseeable future. Feel free to seek it out via DIY means, which are largely safe and peer review tested. (You do have to figure out crypto if you go DIY route, which is bleh (understandable why but still bleh for people to figure out)) I will not be directly linking any DIY store on this page. That isn’t safe for me or them to do.
Erin Reed’s Informed Consent Clinics Map These clinics will get you set up with HRT without a hassle. Planned Parenthood is okay too, mostly. Informed Consent as a model means that you’re told the risks of HRT, but given your HRT without much fuss. No psychologist/psychiatrist. No politics. Just the way it should be, you’re told the health risks and given the medicine you want. It’s simple, it’s beautiful, it should be the default. You should not have to prove your transness to a psychiatrist. There are certain “booby trap” clinics that are just conversion therapy centers in disguise, be aware. Trust your sisters and ask your sisters for safe and solid locations. Erin Reed is one such sister.
You sometimes get prescribed 18g needles for draw. These are pretty big needles that could potentially harm your vial. I recommend in the realm of 21-23g for draw, and 25g for inject. Luer lock 1ml syringes. Your carrier fluid and general vial will dictate how hard it is to push your medicine through a smaller needle. But in general american healthcare is a bit too conservative with needle size, they will have you poking your vial and yourself with bigger needles than necessary.
Injection vid tutorials: Draw IM SubQ
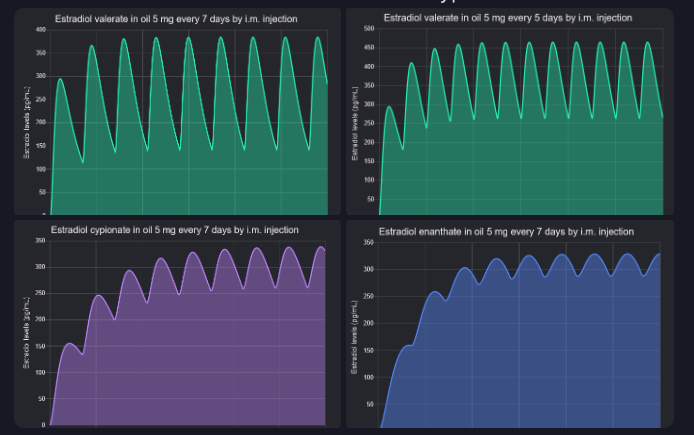
Estradiol Valerate is a popular injectable to prescribe in the american market, more often prescribed than Cypionate. It also has one problem that bugs me: Your hormone cycle is too rollercoaster on it. ESPECIALLY on the 7 days dosage. If you are prescribed 7 days Valerate and you find you have a harder time with emotions and breakdowns, heavily consider opting for 5 day dosage Valerate, or Estradiol Cypionate Injections instead.
Pills (here!)
Transfems will usually need an antiandrogen, a medicine that suppresses testosterone specifically and only, if they use a less effective estradiol such as oral estradiol pills. Cyproterone Acetate is a very good antiandrogen, but banned in USA market because too high of dosages gave men with prostate cancer brain tumors (200mg+ vs the 12.5mg MTF HRT uses) and they didn’t give a fuck about anyone but cis men. Bicalutamide is technically legal but not often prescribed because of a healthcare scare (irrelevant, not worth your attention) and there are some liver concerns.
Smoking will inhibit your estrogen intake with oral estradiol.
Regardless of personal stability and irl situation (usually a wreck anyway for trans people) you should get a therapist for 1-3 years of hrt/social transitioning. It’s a life transition and new and scary stuff is gonna be happening regardless of how accepting those around you are and how accepting of the process you are. My 1st gender doctor strongly advised I get a therapist and I do agree. You’re advised to get a therapist for big life changes, even something as normal as moving. HRT is no different.
I have too much traumas related to therapists. I’ve had one visit in the past two years and I immediately quit. One should not do it stupid like I am. And yes, you can get bad, terrible, or transphobic therapists. Still worth a shot.
HRT. Social transitioning. Therapist. Social safety net (friends, family). Self research into transitioning and all aspects of it, medical, social, history, politics, religion if wanted. Community resources, community centers and gatherings. Needle exchanges/harm reduction programs. Make use of everything you can.
Some opinions begin to crop up here
Oral medication, pills, carry the biggest forms of health risks for transfems. Your body needs to digest the stuff, it goes around your system, most of it gets lost in your stomach, it will go through your liver. Blood clots are the most cited risk (though potentially much less a concern on modern medicine). Doctors and patients will work together in prescribing and getting prescribed higher dosages of oral medication, because patients will often be unhappy with results on minimum dosages and oral medication itself having low efficacy. Thus they will have more health problems on stacking on ineffective medication. 2-8mg oral estradiol (sublingual is good strategy) and 50-200mg spironolactone are normal US healthcare dosages to see for oral medication.
DO NOT FUCKING LET YOUR DOCTOR PRESCRIBE YOU 1MG ORAL ESTRADIOL. ESPECIALLY WITHOUT AN ANTI-ANDROGEN. THIS IS BY FAR THE MOST POPULAR MEDICAL MALPRACTICE I NEED TO FIX IN ADVICE TO OTHERS OFTEN. IT IS A DOSAGE THAT WILL DO NOTHING. IT IS PITIFUL. OFFICIAL HEALTHCARE SOURCES CITE FOR HIGHER DOSAGES THAN THIS. THE ENDOCRINE SOCIETY, THE DSM, WPATH ALL VOUCH FOR HIGHER DOSAGES THAN THIS. OFFICIAL HEALTHCARE IN TRANS CARE IS NOT GREAT AND EVEN THEN THE OFFICIAL HEALTHCARE GUIDELINES ARE HIGHER. THIS IS A STUPID DOSE BY ANY AND EVERY METRIC POSSIBLE AND YET IT GETS PRESCRIBED 5% OF THE TIME. I MOSTLY THINK DOCTORS ARE PUTTING YOU ON A LOW DOSAGE IN THE HOPES YOU CHANGE YOUR MIND.
It is usually more important to lower testosterone than it is to raise estrogen.
Enanthate = Undyclate > Cypionate > Valerate
If one has to be on oral pills, either forced by a doctor or otherwise, at the very least I advocate for 4-8mg sublingual estradiol and 100-200mg Spironolactone for the normal american market trans healthcare. (Sublingual simply means dissolving them under your tongue, it’s more effective that way)
Your general estradiol expectations with scientific and anecdotal evidence are to maximize your effects around 3-5 years of taking HRT. You will not stop feminizing and growing as long as you stay on HRT, breast growth does not stop but it does slow down at some point. Be aware that HRT is a forever medication. Some are surprised by this, expecting to only have to take it for as long as it takes for effects to get Into The Green. But if you get on and get off HRT you will lose some effects that are more temporary, such as libido and emotional changes. It will also have a negative effect on what breasts you’ve grown. Your testosterone will return to Boy level and bring with it Boy effects.
It is usually ideal for most transfem individuals to be on HRT for their whole lives. HRT is a slow acting process, both getting on it and getting off it. If you lose access temporarily for whatever reason, you will Not lose all progress immediately. I am sorry, but doing HRT is a slow process one must have lots of patience on. Even at normal dosages or on injections, it will take years for your effects to show themselves to you and others. Usually. Unless you are very lucky, or perhaps very young.
Progesterone… is a weird one to me. It’s advertised by transfems for transfems to help breast growth. But it seems somewhat scattered for actual results. I personally view it as mildly optional, because it may or may not work for you. It does more than breast growth at least. It can help with body temperature, mental health, libido troubles and enhancement. The prescription dosage typically goes from 100-400mg. I HIGHLY recommend boofing it if you take it. (Taking it rectally) Tests have been done to confirm your body will be getting more of the progesterone that way, and it’s safe to take it that way in capsule form.
The biggest myths in HRT/estrogen
Milk does not help, tea barely helps, beer does not help, soy does not help, Pueraria Mirifica is purely fake for estrogen help, touching paper receipts does not help. These are mostly manosphere falsehoods dreamed up by scammers with something to sell to someone. In general, if a transfem is not already taking and using something to boost estrogen, it does not help or apply estrogenically. The only real way we know to raise and lower hormone levels is via medicine. Also, any estrogen or testosterone you can buy on amazon is fake medicine. It always needs a prescription in the US for the real deal (or DIY from trusted DIY stores in the diy hrt market).
My opinions on Spironolactone are the least well researched and most subjective of my general stack of HRT opinions.
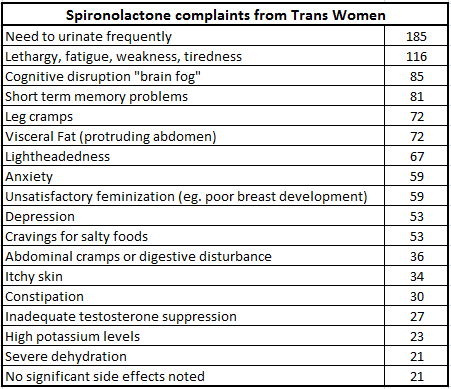
Spironolactone… is a medication I just kinda hate. Studies are showing it might be more harmful than productive. The Extra Peeing Frequency effect is stupid and debilitating and doctors hand wave it too much. It does have notably less efficacy than other antiandrogens. It messes with your blood flow and could prove problematic. It could cause brain fog and generally be worsening one’s depression. It could give you fat on your belly that is very hard to lose. It is an american favorite to prescribe. I personally advocate for getting off it as medication and getting patients onto subjectively better medications. I was on it and found it debilitating and humiliating. I do not personally believe transfems have to be on a medication that humilates them 75% of the time.
What’s Wrong With Spironolactone?
I was below 15ng/dL testosterone for a time and I’d say, be careful. Your goal as transfeminine goals go should not and cannot be to duck your testosterone to 0. Testosterone is still important for basic body functions in transfems; energy level, libido. I personally think with my experience transfems should be on 25-75ngl testosterone, and be trying to measure your dosages to result in such. I was personally happiest with my level at 75ng/dl. You are no less a woman because you have some testosterone in your system.
I recommend highly for further reading the resources of
My own HRT results/journey bluesky thread
Katie’s DIY HRT guide
transfemscience.org, a collection of data and calculators
The many lies of transphobes: A 5 hour video essay
Trans people are highly correlated with autistic individuals. Autism is heavily demonized in our current society, it may help to know Why and Where that comes from: HBomberGuy’s 2 hour video essay on the lies of vaccines falsely correlated with Autism
Being trans is not a bad thing. Being autistic is not a bad thing. Getting vaccines for yourself and others improves the overall health of yourself and society. There is no good reason to demonize any of these things.
In summation, the biggest problems in US trans healthcare I personally see:
- 1mg oral estradiol (sometimes without antiandrogen)
- 18g needles for vial draws, larger needles than necessary in general
- oral pills first, injections rarely advised for
- 7 day dosage valerate
- Clinics that don’t do informed consent
- general refusal on progesterone
- keeping transfems lockstep in 100-200pg/ml estradiol range, fanatically so
- not able/not willing to prescribe CPA or Bicalutamide
- insurance problems with cypionate/needles
- steadfast prescribing Spironolactone, despite issues
- Insurance
- Political Healthcare Climate
- cis people/cis family/cis doctors
- wait lists (you should be seen within a week of deciding you want hrt fyi)
- Insurance

Comments
You can comment on this blog post by publicly replying to this post using a Mastodon or other ActivityPub/Fediverse account. Known non-private replies are displayed below.